

With the recent release of the proposed Medical Aid tariffs for 2017, medical costs were once again thrown into the spotlight.
What are the drivers of increases and what is the prognosis over the next twenty years?
The latest premium increases confirm a long-term trend that medical inflation exceeds CPI by at least two, if not by three, percentage points. Before lambasting the local health care providers, this is an international trend.
Interestingly when the NHS was introduced in Britain during the Atlee administration after WW2, one of their fundamental assumptions was that NHS would tame medical costs and within five years – according to their estimates – it would be below that of CPI for various reasons mainly due to lower usage. The opposite was proved to be true since its introduction.

More than 44,000 people are diagnosed with lung cancer each year in the UK
In the old days when employers bore at least 50% of the cost of the Medical Aid, the effects of these increases was not as pronounced but since the introduction of a fixed salary package by most employers, the employee now has had to face the consequences of rampart medical inflation.
In the cases of pensioners, the effect is much more insidious. Interest rates barely compensate for inflation yet tax could be payable on the interest received. Even in the case where one’s net pension after tax is incrementing at the rate of inflation or CPI, medical inflation will rapidly erode one’s income as evidenced by the table below.
| Effect of Medical Cost Inflation on Pension | ||||||||
| Inflation: | CPI | 6 | Medical | 10 | ||||
| Increasing pension | Static pension | |||||||
| Year | Pension | Medical costs | Remaining | Medical costs as % of Pension | Pension | Medical costs | Remaining | Medical costs as % of Pension |
| 1 | 40 000 | 5 000 | 35 000 | 12.5% | 40 000 | 5 000 | 35 000 | 12.5% |
| 2 | 42 400 | 5 500 | 36 900 | 13.0% | 40 000 | 5 500 | 34 500 | 13.8% |
| 3 | 44 944 | 6 050 | 38 894 | 13.5% | 40 000 | 6 050 | 33 950 | 15.1% |
| 4 | 47 641 | 6 655 | 40 986 | 14.0% | 40 000 | 6 655 | 33 345 | 16.6% |
| 5 | 50 499 | 7 321 | 43 179 | 14.5% | 40 000 | 7 321 | 32 680 | 18.3% |
| 6 | 53 529 | 8 053 | 45 476 | 15.0% | 40 000 | 8 053 | 31 947 | 20.1% |
| 7 | 56 741 | 8 858 | 47 883 | 15.6% | 40 000 | 8 858 | 31 142 | 22.1% |
| 8 | 60 145 | 9 744 | 50 402 | 16.2% | 40 000 | 9 744 | 30 256 | 24.4% |
| 9 | 63 754 | 10 718 | 53 036 | 16.8% | 40 000 | 10 718 | 29 282 | 26.8% |
| 10 | 67 579 | 11 790 | 55 789 | 17.4% | 40 000 | 11 790 | 28 210 | 29.5% |
| 11 | 71 634 | 12 969 | 58 665 | 18.1% | 40 000 | 12 969 | 27 031 | 32.4% |
| 12 | 75 932 | 14 266 | 61 666 | 18.8% | 40 000 | 14 266 | 25 734 | 35.7% |
| 13 | 80 488 | 15 692 | 64 796 | 19.5% | 40 000 | 15 692 | 24 308 | 39.2% |
| 14 | 85 317 | 17 261 | 68 056 | 20.2% | 40 000 | 17 261 | 22 739 | 43.2% |
| 15 | 90 436 | 18 987 | 71 449 | 21.0% | 40 000 | 18 987 | 21 013 | 47.5% |
| 16 | 95 862 | 20 886 | 74 976 | 21.8% | 40 000 | 20 886 | 19 114 | 52.2% |
| 17 | 101 614 | 22 975 | 78 639 | 22.6% | 40 000 | 22 975 | 17 025 | 57.4% |
| 18 | 107 711 | 25 272 | 82 439 | 23.5% | 40 000 | 25 272 | 14 728 | 63.2% |
| 19 | 114 174 | 27 800 | 86 374 | 24.3% | 40 000 | 27 800 | 12 200 | 69.5% |
| 20 | 121 024 | 30 580 | 90 444 | 25.3% | 40 000 | 30 580 | 9 420 | 76.4% |
Drivers of medical cost inflation
Surprisingly administration costs do not feature as major cost driver. From 20 years ago when all claims had to be manually processed, most of these activities are performed electronically. The next quantum leap in cost reduction would be a central database containing all the patients’ details including all the medical tests, medication & medical procedures. This would allow the medical provider to gain a comprehensive view of patient. Instances of overmedication and excessive treatment could easily be determined & monitored.
What is stalling this technological leap worldwide is cost.

One of the drivers of longevity is not necessarily improved nutrition per se but rather improved medical treatment and medication. Even in the case of wars such as those in Afghanistan and Iraq, fewer soldiers died as a result of improved treatment. However this treatment came at huge cost. Similarly with the general population. Scans such as MRI, CT and others have allowed treatment of previous untreatable diseases but this has come at a cost.
Unique to South Africa has been the huge increases in the healthcare service provider’s fees. In particular, I am referring to the specialists. A canoeing friend and urologist in practice, has confirmed this trend. Since 1994, the number of urologists has declined by 50% in South Africa. Its effect has been an unprecedented increase in charge out rates as the shortage of specialists becomes more pronounced.

From a personal perspective, this phenomenon has impacted upon the McCleland household. Janine’s recent back operation will personally cost me R 46,000.
Like the British NHI, South Africa also faces the problem of an increased utilisation of benefits, also a worldwide trend. Instead of accepting that a cold or running nose takes 17 days on average to be “healed”, the modern patient expects antibiotics after 5 days. Even though such a treatment has not more than placebo effect, patient pressure forces doctors to prescribe them.

From a long term perspective – over the next twenty years – the situation is more sanguine. Many of today’s chronic illnesses such as diabetes and fatal diseases such as cancer would have benefited handsomely from gene therapy.
Take the treatment of cancer as an example. Currently the gold standard is chemo, radiation or a combination of both. Yet despite the costs of treatment, in many instances, the ultimate prognosis is death. In other words, the end result of a lengthy treatment merely delays the inevitable. Of all of my family and friends that have been diagnosed with cancer, all but one has died as a consequence of the disease.
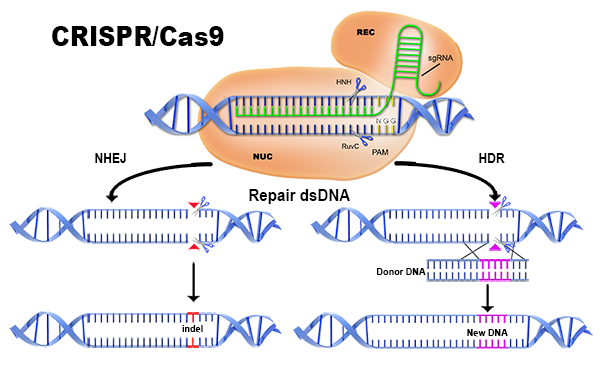
CRISPR Dual Editing Method
Notwithstanding my current derision as to the efficacy of current cancer treatments, a knight in shining armour is on the horizon. All current indications are that a revolutionary treatment known as immunotherapy will revolutionise the treatment of most cancers. Using this procedure, the T-cells are “retrained” to recognise the cancer cells as “mutant” cells. Apparently cancer cells switch off the the T-cells ability to recognise cancer cells as such.
Yet another revolutionary medical technique is in the wings: CISPR. This technique allows medical practitioners to edit ones genes using this simple procedure.

Now for the bad news. In the interim the immunotherapy drugs are prohibitively expensive. Apparently, a patient requires a minimum of four injections at a cost of R 250,000 per injection. Currently no medical aids cover this treatment even on an experimental basis. Moreover even when it is on general release will they be able to afford the cost of treatment.
Ironically if the efficacy of this drug is proven, might not the cost of traditional treatment over numerous years be equivalent to that of four of five injections?

Of greater concern for me, is the imminent introduction of NHS in South Africa. If that were to occur, a significant portion of current contributions would be used to fund uncovered members of the population leaving existing members to fund additional treatment themselves.